The goal of breast reconstruction is to restore one or both breasts to near normal shape, appearance, symmetry and size following mastectomy.
Breast reconstruction often involves multiple procedures performed in stages and can either begin at the time of mastectomy or be delayed until a later date.
Breast reconstruction generally falls into two categories: implant-based reconstruction or flap reconstruction. Implant reconstruction relies on breast implants to help form a new breast mound. Flap reconstruction uses the patient’s own tissue from another part of the body to form a new breast.
There are a number of factors that should be taken into consideration when choosing which option is best:
- Type of mastectomy
- Cancer treatments
- Patient’s body type
Breast reconstruction costs may include:
- Surgeon’s fee
- Hospital or surgical facility costs
- Anesthesia fees
- Prescriptions for medication
- Post-surgery garments
- Medical tests and imaging
Expander Procedures
The most common scenario requires placement of a tissue expander to stretch the skin so that there is enough to properly cover an implant. This process requires 4-6 months, during which time we gradually fill the expander during weekly office visits. Once the adequate size / space have been achieved, we allow 2-3 months for the tissues to stabilize before exchanging the expander for longer lasting gel implants. The decision about the size and type of implant will be made with you at that time.
Flap Procedures
If flap procedures are used, there are a variety of possible techniques depending on which one will provide you with the best result.
Latissimus dorsi flap – In this technique, the muscle, fat, and skin are taken from the back and tunneled to the chest area, where it is placed over an expander. This added skin, fat, and muscle can markedly improve the final outcome versus tissue expanders or implants alone, especially if the patient has undergone radiation.
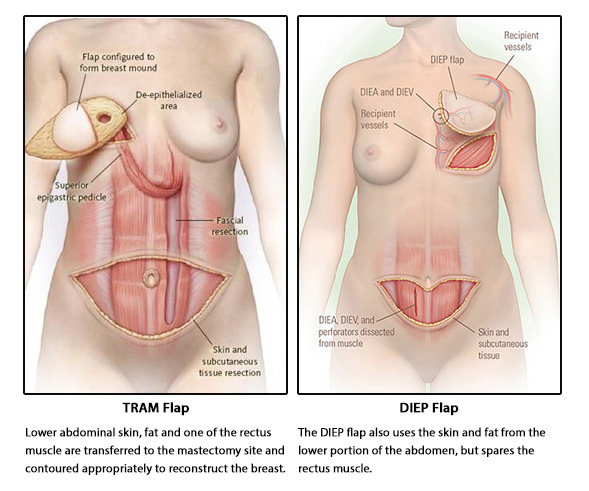
TRAM (transverse rectus abdominus musculocutaneous) flap – In this case, the skin and fatty tissue from the abdomen (which would normally be discarded with a tummy tuck) are used to reconstruct one or both breasts. Most commonly, the tissue is left attached to a leash of muscle which carries the necessary blood vessels. In some cases, only a small segment of muscle and the critical blood vessels are detached from the abdomen and reattached to vessels in the chest with the aid of a microscope (known as a FREE TRAM).
A DIEP flap is similar to a muscle-sparing free TRAM flap, except that no muscle is used to rebuild the breast. (A muscle-sparing free TRAM flap uses a small amount of muscle.) A DIEP flap is considered a muscle-sparing type of flap. DIEP stands for the deep inferior epigastric perforator artery, which runs through the abdomen.
In a DIEP flap, fat, skin, and blood vessels are cut from the wall of the lower belly and moved up to your chest to rebuild your breast. (In a properly performed DIEP, no muscle is cut or removed.) Our surgeon will carefully reattach the blood vessels of the flap to blood vessels in your chest using microsurgery. Because no muscle is used, most women recover more quickly and have a lower risk of losing abdominal muscle strength with a DIEP flap.